Conclusion
Overlaying imaging and ELISA curves increases confidence in exposure trends and helps compare dose/schedule or formulation options without relying solely on post-mortem snapshots.
 Imaging and ELISA alignment builds confidence in exposure trends and supports faster comparisons of dose, schedule, and formulation without relying solely on post-mortem snapshots.
Imaging and ELISA alignment builds confidence in exposure trends and supports faster comparisons of dose, schedule, and formulation without relying solely on post-mortem snapshots.
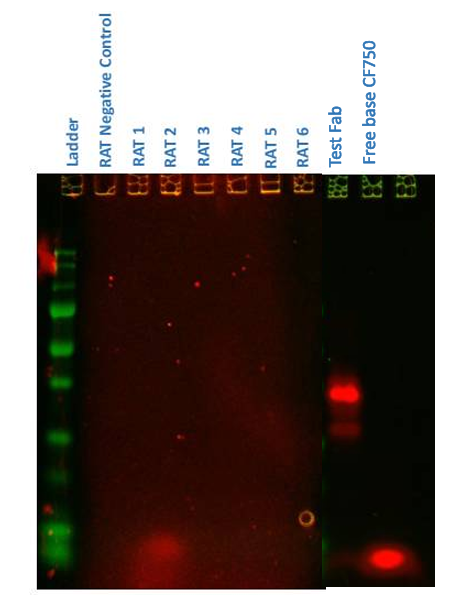
SDS-PAGE identified an early (<24 h) low-molecular-weight fluorescent band (<10 kDa, consistent with free CF750 dye ~3 kDa) in the test Fab, whereas the control Fab showed the expected 25–50 kDa bands.
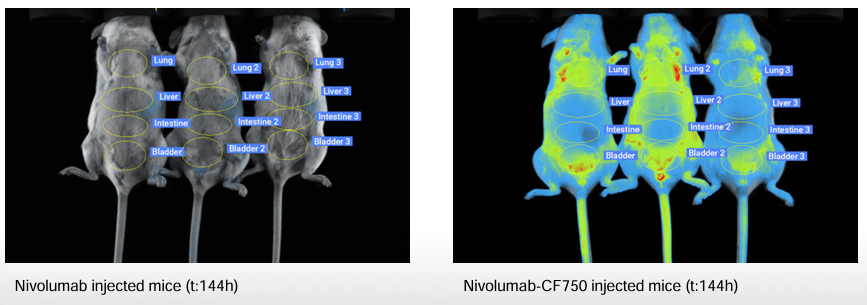
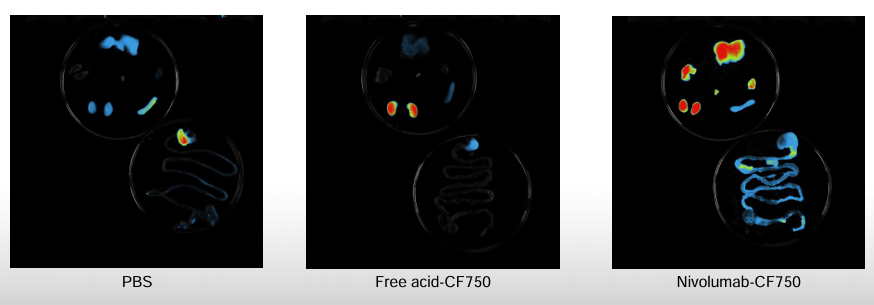
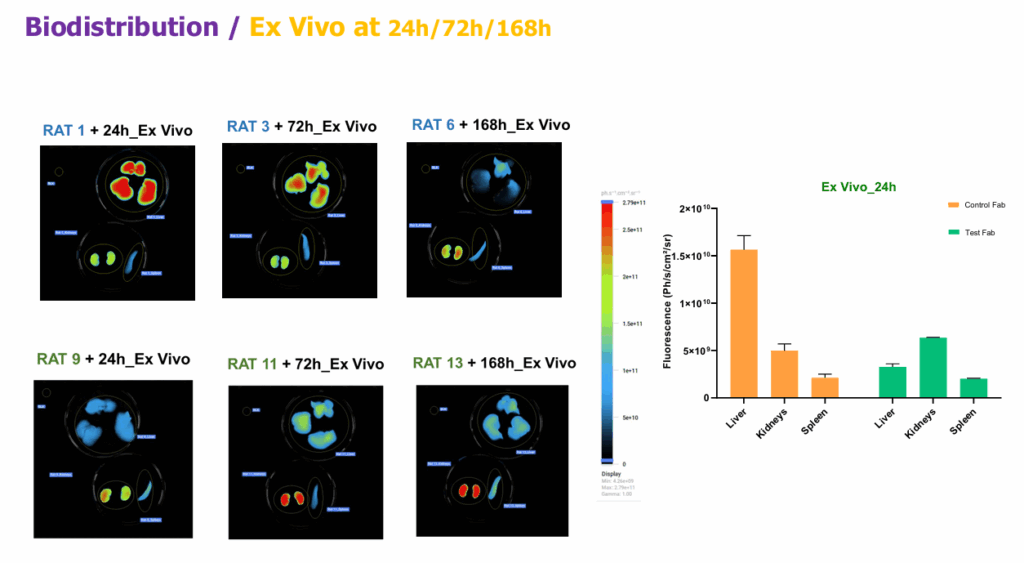
In vivo liver ROIs and ex vivo panels supported absorption and predominant hepatic clearance for the control Fab.
Imaging plus SDS-PAGE reveals <24 h injection-site degradation for the test Fab, while the control is absorbed and cleared hepatically, showing why SC PK designs need site-specific endpoints.
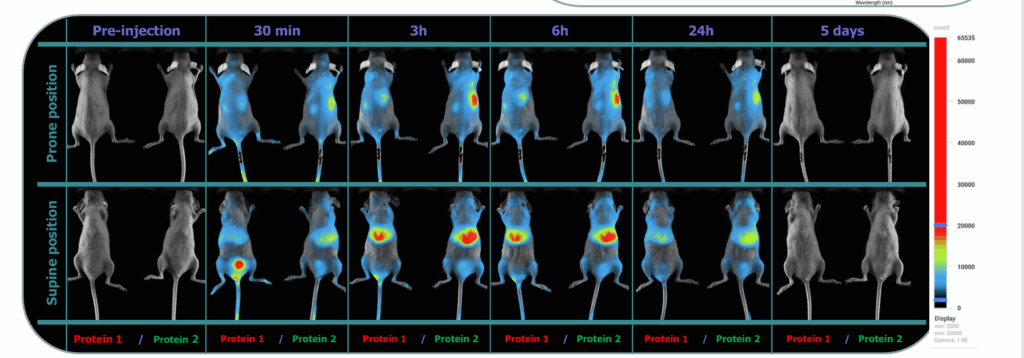
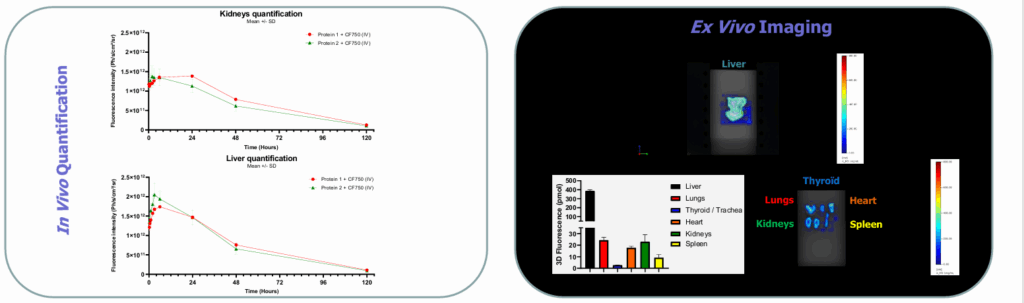
The imager produced clear whole-body signals from early time points through day 5, enabling time-resolved organ ROIs. Liver vs kidney ROIs showed distinct kinetic trajectories, and two model proteins displayed differentiated organ profiles over time.
Ex vivo (6 h) imaging quantified fluorescence across liver, lungs, thyroid/trachea, heart, kidneys, spleen, supporting in-vivo readouts.
This quantitative NIR workflow delivers organ-resolved kinetics with ex-vivo confirmation, often with fewer animals and lower cost than radiolabeled post-mortem designs.
Image-enhanced PK shows where a drug localizes and how it clears, then aligns those patterns with measured concentrations. Together, imaging and bioanalysis turn PK into decision-ready evidence for route, dosing, and formulation.
